

Carpal Tunnel Syndrome, Cervical Radiculopathy, Ulnar Neuropathy and Thoracic Outlet Syndrome all result in hand numbness. Proper diagnosis is essential in choosing effective treatment.
Pins and needles, electrical buzzing and deadness are all descriptions of the sensation people feel when their hands go numb. Up to twenty percent of working people experience on and off numbness of their hands every day. Some are unable to use a hair dryer, put on makeup, navigate a computer mouse, play upper body sports or even grip a steering wheel. Others can’t pick up their own baby or carry groceries in fear of their dropping their precious cargo. Even sleep is at risk, as the arms can become numb upon awakening.
Most of the time, physicians minimize interventions when there is no evidence from electrical testing and no objective signs of nerve compression such as atrophy. Alternatively, misguided professionals often conclude that the source of their pain is nerve compression at the wrist based on equivocal test results, and mistake the numbness for Carpal Tunnel Syndrome. Ineffective steroid injections or unnecessary surgery at the wrist are often wrongly prescribed to those with numbness in their hands. As such, it is imperative to understand the source of the numbness before deciding on the best treatment.
In our clinical experience of over forty years seeing thousands of patients with hand numbness, most people do not have problems with the brain, spinal cord or nerve roots in the spine. As outlined in the textbook of Thoracic Outlet Surgery, now in second edition, it is relatively uncommon for Carpal Tunnel Syndrome to require surgery. Many people with hand numbness have either a pinched nerve at the elbow, ulnar neuropathy, or a pinched nerve along the pathway from the neck through the shoulder, Thoracic Outlet Syndrome.
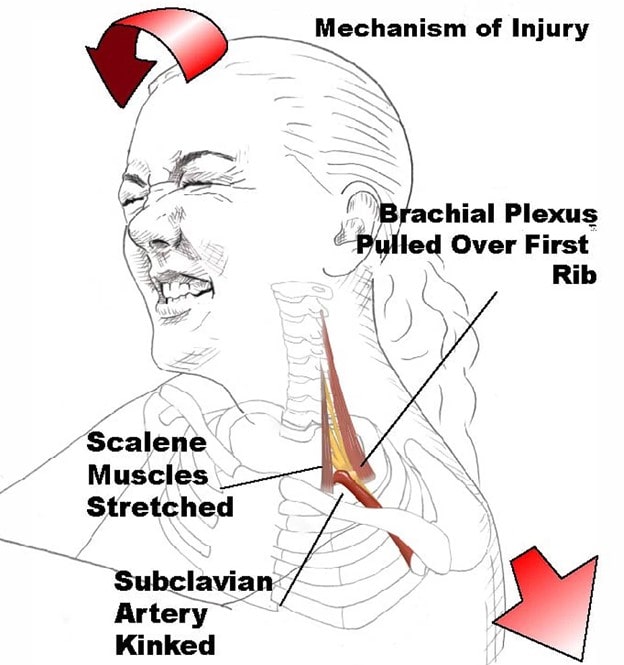
Upper extremity sports such as weight lifting, swimming, tennis and volleyball can produce repetitive injury to the bundle of nerves going through the shoulder resulting in chronic and recurring hand numbness and pain. Other repetitive exposures including computer work and playing musical instruments may have similar results. In some cases, an automobile accident or a fall results in an acute injury to the neck and shoulder which may also eventuate in a chronic Thoracic Outlet Syndrome. In these cases of either acute injury or repetitive exposure, there is often an underlying anatomical predisposition where an extra top rib or fibrous band narrows the nerve and vessel entry portal to the shoulder pathway. Any additional injury related tension of the surrounding muscles, such as the scalene muscles causes a critical obstruction for nerves and vessels with resulting symptoms.
Testing is simple but often misunderstood. Raising the arms up in a “bank hold up” position and then slowly opening and closing the hands for a minute is a good screening test. An average person will be able to do this test quite easily with nothing more than slight fatigue or weakness. In this position, even some people will temporarily lose their wrist pulse. This result is expected, otherwise, we would have to expect a world without hair brushing, tooth brushing, swimming, weight lifting and Sandy Koufax would have been pitching underhanded. The key observation with Thoracic Outlet Syndrome is that this sort of activity will provoke their typical hand numbness, fatigue and pain to a significant degree.
Proper diagnosis is critical in order to avoid unnecessary surgery that would have been appropriate for other conditions. A particularly problematic challenge for the patient and for the professional is that with acute or chronic injuries, there may be coexisting pain generators such as a shoulder tendinitis. Fortunately, proper ergonomic changes, physical therapy, career adjustments, injection treatments and appropriate surgery are all possibilities that may be successful when chosen on an individualized basis.
-Sheldon Jordan MD